MRI Protocol Tool V2
Body-system and indication-based MRI protocol selector. Covers brain, spine, MSK, body, and vascular. Internal access required.
Internal
Access Required
Clinical Neuroradiology
Central Sulcus provides clinical neuroradiology tools, structured reporting aids, and educational resources built for the complexity of modern neuroimaging.
Clinical Tools
Each tool runs entirely in your browser — no login, no installation, no data leaves your device. Designed for clinical use, accessible from any hospital computer.
Downloads
Clinical reference PDFs and working files. Password-protected sections require internal access.
About
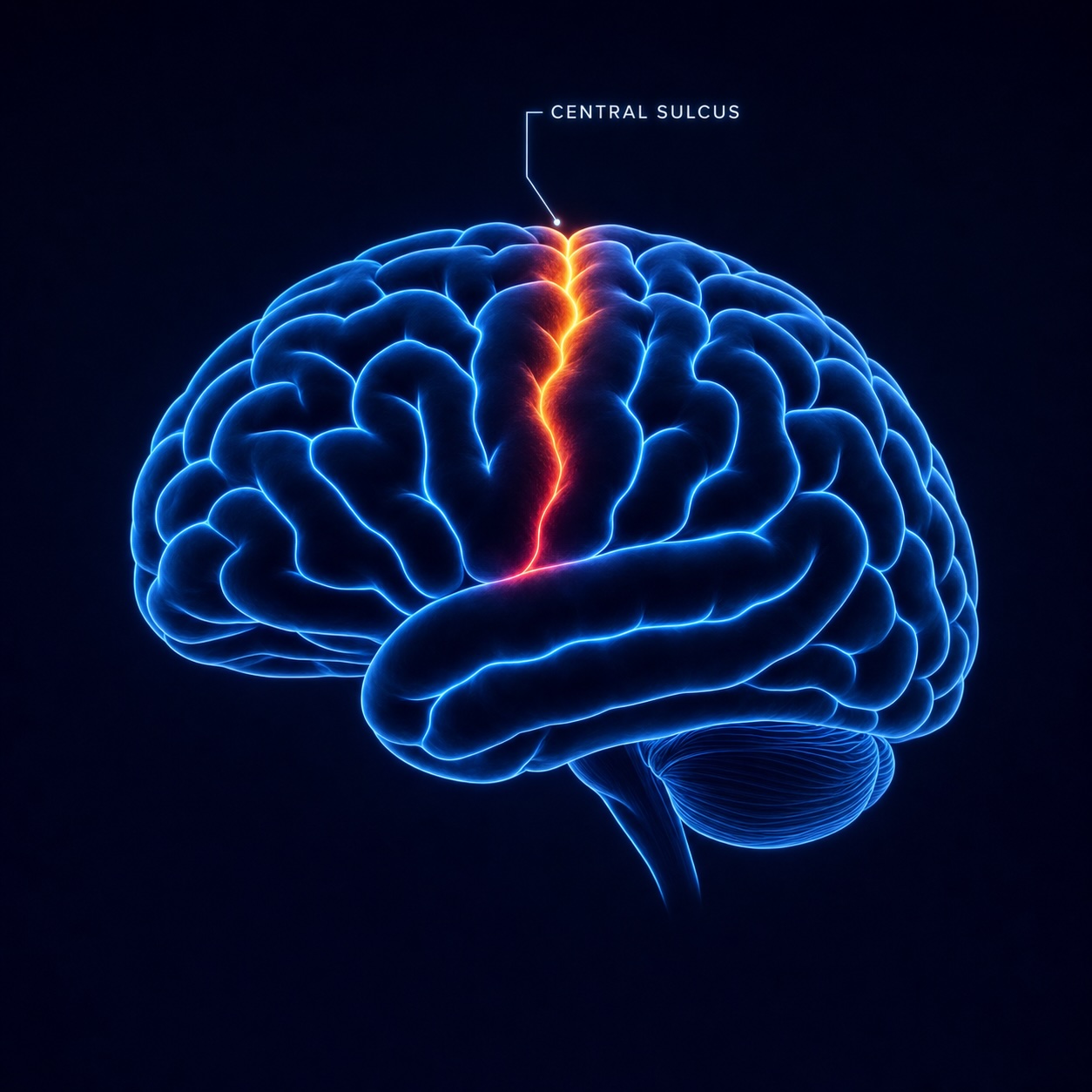
The central sulcus — the landmark fissure dividing the frontal and parietal lobes — sits at the boundary between motor output and sensory processing. It is one of the most reliably identified structures in neuroimaging, and one of the most important to get right.
This site takes its name from that landmark. The tools here are built around the same idea: clear boundaries, reliable structure, and precision in the details that matter.
Each tool was developed from real clinical workflows — tumor board tracking, structured reporting, imaging protocol selection — and refined for the way radiologists actually work. Every tool runs entirely in the browser; no data is transmitted or stored.
Quick Reference
Sagittal brain anatomy most relevant to neuroimaging interpretation.